


In recent years, a lot more has been written about how menopause’s hormonal changes can have certain physical and mental effects. But how much do we know about how those changes can affect eye health? And is what we know about menopause and menopausal hormone therapy (MHT) enough to substantiate changes to our clinical practice?
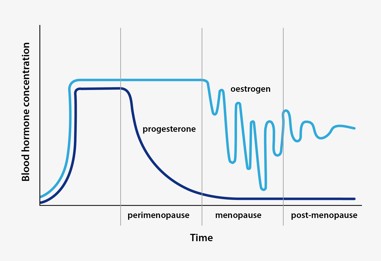
Menopause is the biological process ending monthly menstruation, resulting in the loss of ovarian follicular function and thus a woman’s ability to reproduce. It typically happens between the ages of 45 and 58, when the body’s production of oestrogen and progesterone decreases. Oestrogen doesn’t drop dramatically at first but tends to surge and drop more like a wave before resulting in a permanent reduction (Fig 1). It is this hormonal fluctuation (in the context of low progesterone) that causes menopausal symptoms such as hot flushes, sleep and mood disturbances, weight gain and muscle and joint aches. It is also worth noting, however, that a relative increase in androgen levels can cause some women to experience additional symptoms associated with hyperandrogenemia, including facial hair growth and scalp hair loss.
Some women try to ameliorate the effects of these hormonal fluctuations with menopausal hormone therapy (MHT), previously known as hormone replacement therapy (HRT). MHTs differ in their levels of oestrogen, progesterone and sometimes even testosterone. There are also different modes of delivery, ranging from tablets to creams and intrauterine devices (IUDs). Use of MHT is complicated and its indication needs to be made on an individual basis. A meta-analysis conducted in 2019 found an association between some types of MHT, duration of MHT use and incidence of breast cancer¹. However, current international recommendations state MHT is safe and effective for most healthy females and the benefits outweigh the risks for those with significant menopausal symptoms.
Glaucoma
There is an ongoing debate about whether menopause should be considered a sex-specific risk factor for glaucoma. One meta-analysis found an inverse linear relationship between age of onset of menopause and the risk of developing open angle glaucoma (OAG)2. This could indicate that early menopause (occurring in those aged <45, which can be due to chromosome issues, autoimmune conditions such as thyroid disease, epilepsy or individual genetics, or lifestyle factors such as history of smoking and low BMI) can be associated with an increased risk of developing OAG.
Preclinical rat studies found induction of ocular hypertension, larger vision loss (as measured by optomotor response) and retinal ganglion cell (RGC) loss (as measured by OCT) was associated with surgically induced menopause via ovariectomy3,4. One study also found oestrogen administration played a protective role in RGC layer integrity5; however, more studies are needed to confirm the relevance of oestrogen in glaucoma prevention.
Other animal studies investigated the effects of menopause on aqueous outflow and ocular compliance (related to the elastic properties of the sclera and cornea as well as blood circulation) to better understand whether these factors could play a role in the association between menopause and increased intraocular pressure (IOP). They found menopausal rats had a 34% decrease in aqueous outflow and 19% increase in ocular compliance when compared to controls6, which could result in some of the physiological factors associated with glaucoma. Overall, the literature seems to indicate that in animal studies, surgically induced menopause is related to increased IOP, increased aqueous outflow resistance and ocular biomechanics - factors we know can be associated with glaucoma. Thus, it could be possible that menopause sets the stage for glaucoma to develop5.
Human studies are limited. One found that in postmenopausal women there was an increase in IOP and biomechanics measures (resistivity index of vasculature, measures of retrobulbar blood flow), while MHT was associated with a decrease in IOP and resistivity index7. However, a far more recent meta-analysis and systematic review of randomised control trials (RCT) found that MHT did not result in a significant reduction in IOP⁸.
Studies have shown that early menopause doubles the risk of developing glaucoma, said Dr Noor Ali, a Canberra-based specialist in glaucoma, retinal disease and uveitis. “In age-matched female patients, those who have undergone menopause had average IOPs of 1.5-3.5mmHg greater than their premenopausal counterparts,” she said. “In addition, in vitro studies have suggested greater RGC loss after menopause5. While there are many confounding factors to be considered, as a practical note, postmenopausal women would benefit from a full assessment if there are any signs (of glaucoma) in screening.”
Ocular surface disease
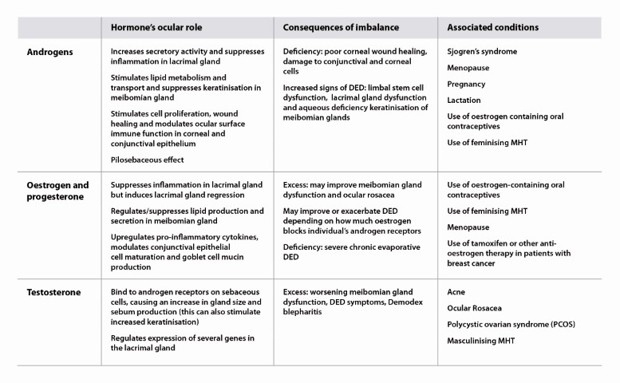
The TFOS DEWS II workshop report labels menopause status as an inconclusive non-modifiable risk factor for dry eye disease (DED)9. Understanding the role of androgens, oestrogen, progesterone and testosterone on the ocular surface can help us see why hormonal changes that mark menopause do not have a generalisable effect on DED (Table 1). Changing levels of different hormones will have different influences on factors contributing to the exacerbation or relief of DED. For example, decreased oestrogen levels may promote lipid production in the meibomian glands but suppress goblet cell mucin production. Thus, MHT can be both beneficial and harmful to DED patients.
Using basal and reflex Schirmer test and tear break up time (TBUT) results, one study found menopause increases the incidence of DED, but MHT can decrease its incidence7. Other studies found similar improvements associated with MHT in postmenopausal women when assessing DED symptoms12. It is important to note, however, that large-scale clinical trials in this area have not been performed.
Another paper suggested MHT could improve ocular surface function in postmenopausal women (especially in those whose menopause onset was before the age of 55). The systematic review and meta-analysis found that the improvement noted in oestrogen-only MHT was greater than that observed in MHT combining oestrogen and progesterone. Signs measured were TBUT, basal and reflex Schirmer test, plus corneal staining scores8. Interestingly, one study reported that greater doses of both oestrogen-only and oestrogen-plus-progesterone MHT resulted in worse DED symptoms in patients than in those who used lower doses of the same MHT therapies13. It was suggested the conflicting findings could be related to selection bias and patient subjectivity reporting/perception of symptoms.
Dr Stuti Misra, an optometrist-scientist and senior lecturer in the ophthalmology department at the University of Auckland who has researched this area, agreed study findings are contradictory when it comes to the benefits or drawbacks of MHT for patients with or without dry eye symptoms. For example, this can depend on the patient's age¹⁴, she said. “There is no one-size-fits-all with MHT. For example, both hyperandrogenemia and androgen deficiency can occur during menopause. Each condition requires different treatment options and, therefore, the effects of each treatment will differ significantly.”
The fluctuations in hormone levels during menopause also lead to varying levels of symptom relief or aggravation, said Dr Misra. “The timing of treatment is also crucial. Oestrogen can relieve symptoms early on, yet it can lead to adverse effects in later stages¹⁵. Interestingly, a large study of over 25,000 postmenopausal women using oestrogen-only MHT presented a greater risk of DED¹⁶.”
It’s difficult to comment on MHT and DED due to the lack of well-designed, methodologically robust longitudinal clinical trials, she added, suggesting that eyecare practitioners (ECPs) obtain a detailed history of DED symptoms during a patient’s regular menstrual cycle. “The exact history will create a database of patients' dry eye symptom history.”
Cataracts
There is some evidence suggesting an older age of onset for menopause is associated with decreased risk of cortical cataract, while postmenopausal oestrogen use is associated with a decreased risk of more severe nuclear sclerosis¹⁷. This could mean that oestrogen (endogenous/exogenous) could have a protective effect against cataract development. However, it’s important to note conflicting findings. For example, one study performed regression analysis to calculate the relative risks of various lifestyle factors (including the use of hormone therapy) in an individual developing a cataract that required surgery. MHT showed little if any association with reducing the risk of cataract development¹⁸.
“Menopause and cataracts, though seemingly unrelated, have intriguing links, primarily through hormonal changes and ageing processes,” said one Australasian cataract specialist who didn’t wish to be named. Intrigued, however, he decided to discuss the matter with ChatGPT and review the AI chatbot’s responses. These are the results:
In conclusion, the surgeon surmised, the links are intertwined and thus confound our ability to truly, independently assess the role of menopause in cataract development and progression, as well as the effect of MHT on cataract progression.
Macular degeneration
According to one study, an older age of menopause onset may be associated with geographic atrophy, while another found the risk of developing neovascular age-related macular degeneration (AMD) was reduced by 70% in women using MHT and 40% in women who’d used MHT¹⁹. But these were isolated studies. Large, population-based studies have failed to consistently find the female gender as a risk factor for AMD when controlled for age, especially given women have a longer life expectancy, so we are clinically more likely to see more older women with AMD.
Dr Rachel Barnes, a specialist in retinal and inherited retinal disease, said she believes menopause is too complex and confounded by other factors to really incorporate clinically. “Although, of course, you should always take a full medication history when evaluating a new patient, which would include MHT.”
There appears to be a number of epidemiology studies in the literature, however, which demonstrate an association with MHT, the length of reproductive life or sex with the prevalence of various forms of AMD. But there is no consistency in the direction of the association, with some showing an apparently protective effect and others the opposite, said Dr Barnes. “I think at the end of the day, the strongest risk factor for AMD is age. Women tend to live longer and postmenopausal – ageing – women may be prescribed MHT, so often an apparent association disappears when you control for age. I think it is really important to investigate these potential links, but nothing I have read so far would make me change someone’s management with respect to MHT and AMD.”
The ECP’s role
Overall, it is difficult to separate the role of menopause and MHT in ocular pathology from confounding factors. For this reason, there is not enough justification to change our standardised guidelines when it comes to clinical workups for the ocular presentations discussed above. However, asking about a patient’s menopause status, age of menopause onset and use of MHT could be useful during history taking and help fill in the clinical picture. MHT also comes in different formulations and modes of delivery, so we should look up each particular MHT to help us understand the potential effects on the patient’s body and their eyes.
References

Australia-based optometrist Layal Naji is a lecturer of optometry at the University of Canberra, a co-founder of the outreach optometry clinic at the Asylum Seekers Centre in Newtown, Sydney, and a regular contributor to NZ Optics.