Optimal outcomes from cataract surgery require accurate pre-operative measurement of corneal curvature. Patients are increasingly expecting perfect outcomes, regardless of the health of their eyes. Attaining excellent unaided visual acuity requires a lot more consideration and planning in eyes with irregular corneal astigmatism. Eyes with keratoconus, corneal scars and those that have undergone older keratorefractive procedures, such as radial keratotomy, are especially difficult to measure consistently and to achieve predicted outcomes routinely.
However, with appropriate refractive planning and management, these eyes can provide the most satisfying outcomes. I present one such case below and discuss small-aperture intraocular lens (IOL) technology as a still relatively novel option for treating the growing number of patients who have undergone early, corneal refractive procedures and now require cataract surgery.
The case
A 63 year-old woman with declining best corrected visual acuity (BCVA) in her left eye, progressive myopia and variable astigmatism. She had undergone bilateral radial keratotomy (RK) surgery for myopia, 20 years previously, followed by arcuate keratotomies (AK) for residual astigmatism and further myopic laser in situ keratomileusis (LASIK) surgery 10 years later.
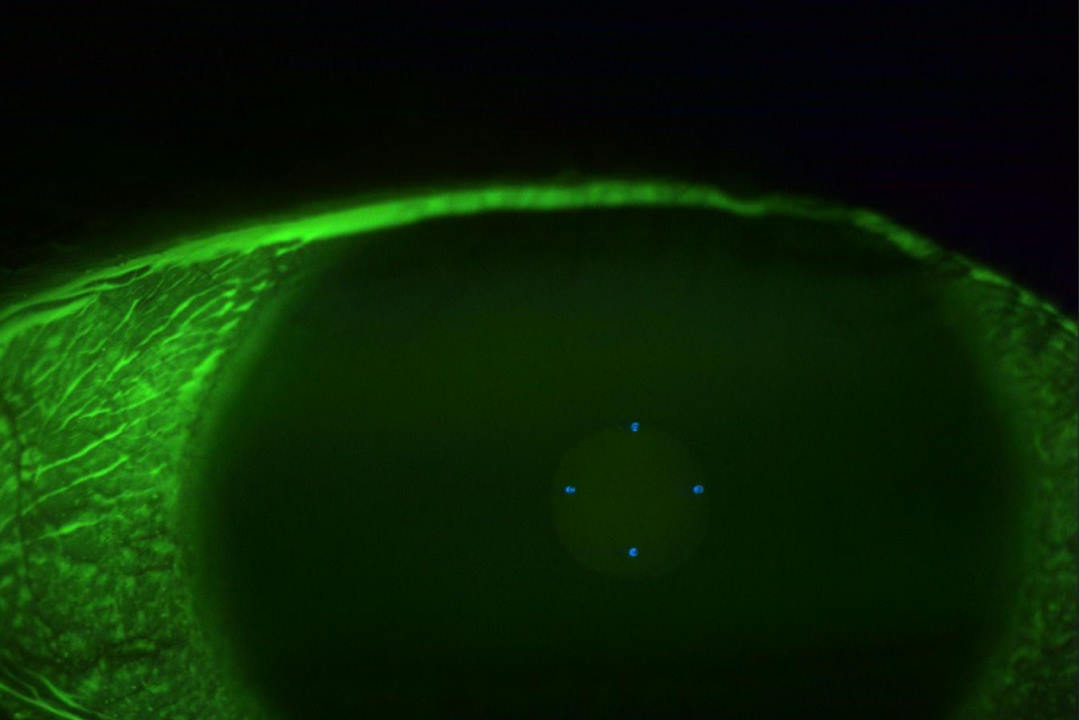
Unaided distance visual acuity (UDVA) in her left eye was 6/48 and BCVA was a poor quality 6/24. She had 10 radial, near-full-thickness RK cuts in each cornea approaching her visual axis, more peripheral AK scars and a peripheral, circumferential LASIK scar. She had also developed a moderately dense nuclear sclerotic cataract with an early posterior subcapsular component (Fig 1).

Fig 1. Intraoperative view of RK scars and cataract
Her posterior segment was healthy. Her anterior keratometry measurements varied widely between devices, which was expected given the various diameters of corneal measurement and the effect of her RK incisions. However, they also varied when measured multiple times on the same device. Following attempts to optimise her ocular surface, she returned on a subsequent day for repeat keratometry and also showed quite marked diurnal variation in her measurements. Her corneal tomography (Fig 2) displayed irregular corneal astigmatism, as would be expected after undergoing so many different and relatively early corneal procedures.

Fig 2. Anterior corneal topography showing irregular astigmatism
Treatment and results
Although there were a number of treatment options available to improve vision quality, in this case, due to the presence of cataract, any treatment needed to include lens replacement surgery. Given, the patient’s previous RK and LASIK, I didn’t wish to perform any further laser ablation treatment. Topographically guided phototherapeutic keratectomy (PTK) is an excellent and safe method to regularise corneal shape in many situations1. After two previous procedures, however, there is a risk of inflammation and given the variability in pre-operative measurements, it would be like trying to change the shape of a moving target. Both the magnitude and axis of the patient’s astigmatism was also variable, so implantation of a toric IOL would be imprecise and it was unlikely to provide a satisfactory vision quality solution.
So, we decided to implant an IC-8 (Acufocus) small aperture IOL. This lens was originally designed to give extended depth of focus as a presbyopia solution, but I believe its true strength lies in therapeutic cases such as this. The IC-8 is a single-piece acrylic lens embedded with an opaque mask measuring 3.23mm in diameter with a central 1.36mm diameter aperture. It can be implanted in the non-dominant eye to give monovision, with a natural range of good visual acuity based on the pinhole effect. In eyes with irregular astigmatism, the mask blocks peripheral aberrated light rays from degrading image quality and the collimating effect of the central aperture provides a focused image despite moderate residual corneal astigmatism.
We discussed the pros and cons of using this IOL, including the limited information about lens power calculation following multiple refractive procedures. A gradual and ongoing hyperopic shift is expected in eyes with RK, so we aimed for a moderately myopic target. Implantation surgery went smoothly. This IOL requires a fairly large 3.5mm incision which I sutured (Fig 3).
The patient had immediate vision improvement. At one month, her UDVA was 6/6 and she could read N6 comfortably, unaided. We were both very happy with the outcome and she is considering undergoing the same treatment for her second eye.
Discussion
The IC-8 small aperture IOL is an excellent additional string to the bow of cataract surgeons. Eyes which have had previous RK are plagued by variable keratometry, unpredictable long-term refractive findings, variable astigmatism and gradual hyperopic shift. These eyes are difficult to work with in all respects. Thankfully RK as a procedure has virtually died out worldwide, but a large number of these patients are now presenting for cataract surgery and creating headaches for surgeons.
There are two major benefits for IC-8 IOL in this group of eyes2. Firstly, they tolerate a wide range of spherical refractive outcomes owing to their depth of focus. This means small errors in outcome, due to inconsistent measurements or hyperopic shift, will still allow good visual outcomes. Secondly, they provide excellent quality of vision with up to 1.5D of uncorrected astigmatism so a precise toric IOL implantation axis is not required.
From experience, I personally prefer trifocal IOLs when trying to achieve spectacle independence in eyes with regular corneas. I see the IC-8 as more of a therapeutic option for irregular corneas3. The visual aberrations induced by traditional multifocal IOLs can compound pre-existing aberrations from an irregular cornea and should be avoided in such cases.
While the IC-8 has been shown to be a very good IOL in terms of presbyopia solutions4, the potential to make vision slightly dimmer concerns me for routine use in normal eyes for patients wanting enhanced vision5.
In non-routine eyes with irregular astigmatism such as in this case, communication is paramount. Discussing the pros and cons of each option takes time, but these longer pre-operative appointments allow both the patient and doctor to ensure they are on the same page about goals and set realistic expectations. This is especially important in multi-step procedures, such as the combination of corneal cross-linking and topographically guided regularisation, and laser refractive ablation.
Unfortunately, sometimes we have to say ‘no’ to certain requests, such as multifocal intraocular lenses (IOLs) or LASIK due to irregular corneal astigmatism, though most patients are happy this decision is being made for their long-term benefit. Patients who have had previous laser vision correction procedures are known to present earlier for cataract surgery and their high expectations can be challenging, especially if they have corneal irregularity. While regularising corneal shape with laser ablation can be extremely satisfying, there are some eyes where it’s unwise to do so despite many patients expecting a laser can fix just about anything these days.
Not all corneal scars are amenable to laser treatment either. Deep corneal depressions require a very deep ablation to provide a regular surface and this can destabilise the cornea as well as induce aberrations. There is certainly still a role for conservative options, such as contact lenses in such eyes. Modern contact lens materials and designs allow some patients to avoid further surgery altogether.
In conclusion
There are no particular barriers to surgeons using the IC-8 IOL other than familiarity. Given the excellent patient outcome in this case, I would strongly encourage its use in similar cases.
References
Dr Ben LaHood is a consultant ophthalmologist at Eye Institute specialising in laser refractive and cataract surgery. He has published and presented widely on his specialist interest of astigmatism management.