A previously healthy 29-year-old New Zealand European female was referred with a four-week history of blurred central vision in the left eye and headaches after returning from her honeymoon in Italy. She’d had two episodes of blue and white flashing lights and the colour was desaturated in her left eye. Earlier the same day, the patient had seen a neurologist who considered the symptoms were not suggestive of demyelinating disease. During childhood, convergence exercises were implemented and Irlen lenses had been prescribed. Medical history was unremarkable but there was a positive family history of multiple sclerosis, with the patient’s mother affected.
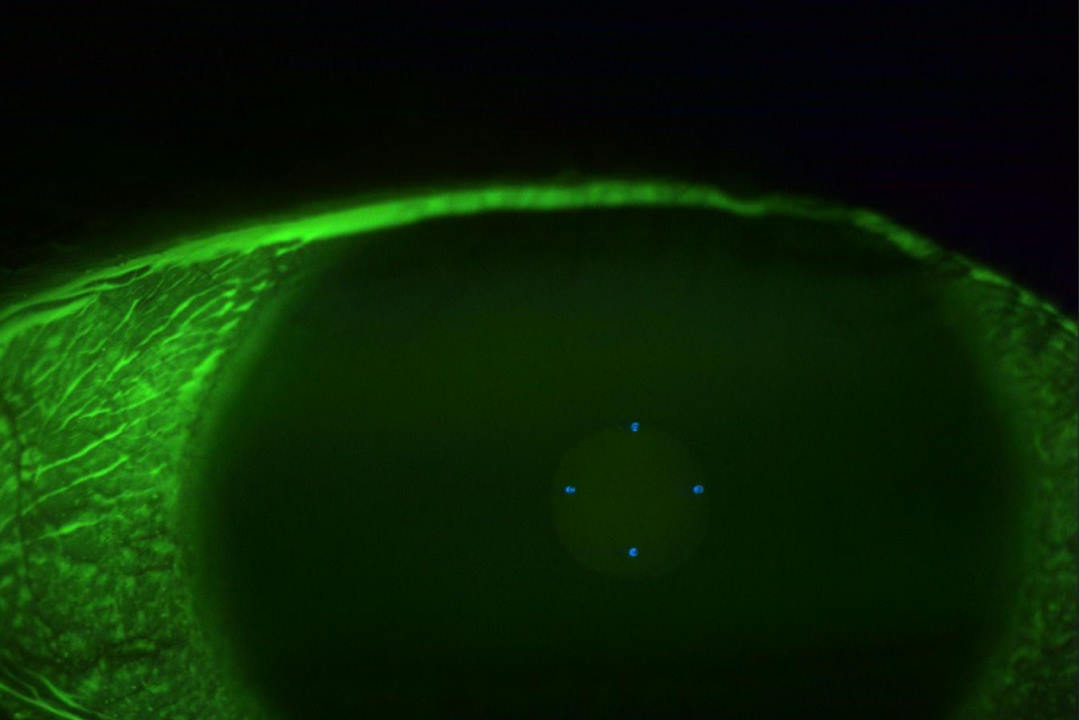
On examination, right and left unaided visual acuities were 6/6. There was no relative afferent pupillary defect and visual fields were full to confrontation. All Ishihara colour vision plates were correctly identified when each eye was tested independently. Anterior segment examination was unremarkable in both eyes and there was no intraocular inflammation. Retinal examination showed a remnant of glial tissue at the right optic nerve but no other abnormalities. In the left eye there was inflammation adjacent to the nasal margin of the optic nerve head (Fig 1). Peripheral retinal examination was unremarkable and there was no vasculitis.
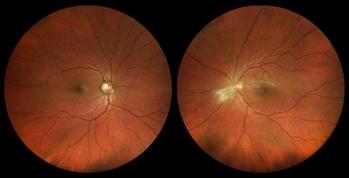
Fig 1. Widefield colour fundus photograph of the right eye shows a glial tissue remnant on the nasal aspect of the optic nerve head. Fundus photograph of the left eye shows inflammation adjacent to the nasal margin of the optic nerve head
Automated visual field testing was normal for the right eye and the left showed patchy nonspecific changes temporally and in the superior field (Fig 2). Macular OCT scans were normal. The OCT retinal nerve fibre layer thickness scans demonstrated the glial tissue remnant at the right optic nerve head and optic nerve head swelling in the left eye (Fig 3).

Fig 2. Humphrey visual field of the left eye showing patchy, nonspecific changes temporally and in the superior field. The right field is normal

Fig 3. The OCT retinal nerve fibre layer thickness scan of the right eye is normal. The OCT scan of the left eye demonstrates optic nerve head swelling
Diagnosis
The differential diagnosis in this case includes:
Targeted investigations were requested, with the following results:
A diagnosis of toxoplasmosis with a focus of inflammation adjacent to or within the left optic nerve head was made. Treatment with cotrimoxazole 960mg orally twice daily for four weeks was commenced and follow-up arranged at another centre due to the patient relocating away from the area the following day.
Ocular toxoplasmosis
Ocular toxoplasmosis is an infection caused by the intracellular parasite Toxoplasma gondii. It affects both the retina and the choroid and is a common cause of posterior uveitis that can significantly impair vision if not managed effectively.
The definitive host of T. gondii is the domestic cat, with humans and other mammals being intermediate hosts who are subject to two routes of infection. Acquired infection is more common (two-thirds of cases)1 and occurs when humans ingest toxoplasma oocysts in contaminated food or water or eat undercooked meat containing tissue cysts2. Congenital infection (one-third of cases)1 occurs when a pregnant mother transmits infection to the foetus and may cause congenital malformation and foetal death. Congenital systemic infection occurs in up to 50% of infants with up to 90% of these demonstrating ocular disease. Risk of transmission is highest if the mother is infected during the third trimester3.
Symptoms and signs vary depending on the severity, size and location of infection and include:
Active toxoplasmosis appears as retinochoroiditis with a white retinal lesion with ill-defined borders and overlying vitritis. While anterior segment inflammation may or may not be present, vitritis is almost always present. Vasculitis is not a common feature but may be present adjacent to an active lesion. Optic neuritis may occur but is generally considered an atypical feature. Uncommonly, punctate outer retinal toxoplasmosis (PORT) occurs as small multifocal lesions in both the deep retinal layers and retinal pigment epithelium and is best delineated using OCT, fundus autofluorescence, OCT angiography and dye-based angiography (FFA and ICG)4.
Diagnosis is usually clinical. Serologic testing is useful in atypical cases, such as the one presented, and is useful to support diagnosis.
Management
In most immunocompetent patients, toxoplasma infection is asymptomatic, does not require treatment and is usually self-limiting, resolving within 4–8 weeks. In immunocompromised patients, however, the infection is usually more severe. Moreover, there is a lack of evidence to support routine treatment of acute toxoplasma retinochoroiditis5 and treatment remains controversial. However, treatment is indicated in the following situations:
Classic treatment consists of oral pyrimethamine, sulfadiazine and folinic acid with prednisone 1mg/kg from day three, tapered over 2–6 weeks. This regime is not now routinely used, given the risk of leucopaenia and thrombocytopaenia, and classic therapy is not safe in pregnancy3. The rationale for corticosteroid use is to suppress inflammation and limit chorioretinal tissue damage.
An alternative regime demonstrating similar efficacy is co-trimoxazole 960mg orally twice daily for four weeks with prednisone 1mg/kg started after three days7-8. Other regimes include clindamycin (300mg every six hours), azithromycin (loading dose 1g then 500mg once daily for three weeks), spiramycin (1g twice daily), atovaquone (750mg every six hours for 4–6 weeks) or minocycline (100mg every 12 hours for 4–6 weeks) either singly or in combination with pyrimethamine (loading dose 100mg then 25mg twice daily for 4-6 weeks), folinic acid (15mg once daily) and prednisone. Pseudomembranous colitis may complicate treatment with clindamycin4.
If systemic treatment is contraindicated, intravitreal clindamycin 1mg (with or without dexamethasone 400µg) is an acceptable alternative9.
Visual prognosis varies depending on retinal location, extent of retinal damage and promptness of treatment when infection is sight threatening. Early diagnosis and appropriate treatment are associated with good visual outcomes. However, permanent vision loss may occur in severe cases or those with delayed treatment, particularly if the macula is involved. Recurrence can also impact visual prognosis.
References

Dr Andrew Thompson is a consultant ophthalmologist with special interests in cataract and refractive surgery, glaucoma and medical retinal disease. He consults and operates at Tauranga Eye Specialists and is the Censor-in-Chief of RANZCO.