Dry eye disease (DED) occurs more frequently in women than in men and it’s recognised that hormones play an important role in the health and preservation of ocular surface tissues. Studies have demonstrated a direct link between hormones and susceptibility to DED1-4, linked to the presence of sex-steroid receptors on the meibomian glands - androgens appear to increase the synthesis and secretion of lipids from the meibomian glands, while oestrogen appears to cause a decrease in lipid production5.
The exact link between hormone levels and DED, however, is uncertain with some studies finding higher levels of both testosterone and oestrogen in women with dry eye1 while others found lower levels of both hormones in post-menopausal women with DED. One thing is evident: altering hormones has an impact on ocular surface condition. Therefore, drugs that alter hormone levels often have an effect on ocular surface disease.
Finasteride, sold under the brand name Propecia, is a 5-alpha reductase inhibitor used for the treatment of male pattern baldness and prostate disease. The drug inhibits the conversion of testosterone into dihydrotestosterone (DHT), decreasing the action of DHT (the androgen responsible for hair loss) on its target tissues. Treatment with finasteride helps restore the amount of circulating testosterone in men, increasing levels by 8-10%6.
Along with these reported benefits, however, at least one study has demonstrated an increased prevalence of DED in men treated for benign prostate hyperplasia 7, and, increasingly, men presenting to our clinic with DED symptoms report a history of finasteride use. The main symptoms include gritty, tired, red eyes, often worse after sustained close work. Patients are also usually frustrated that ocular lubricants provide only transient, if any, relief.
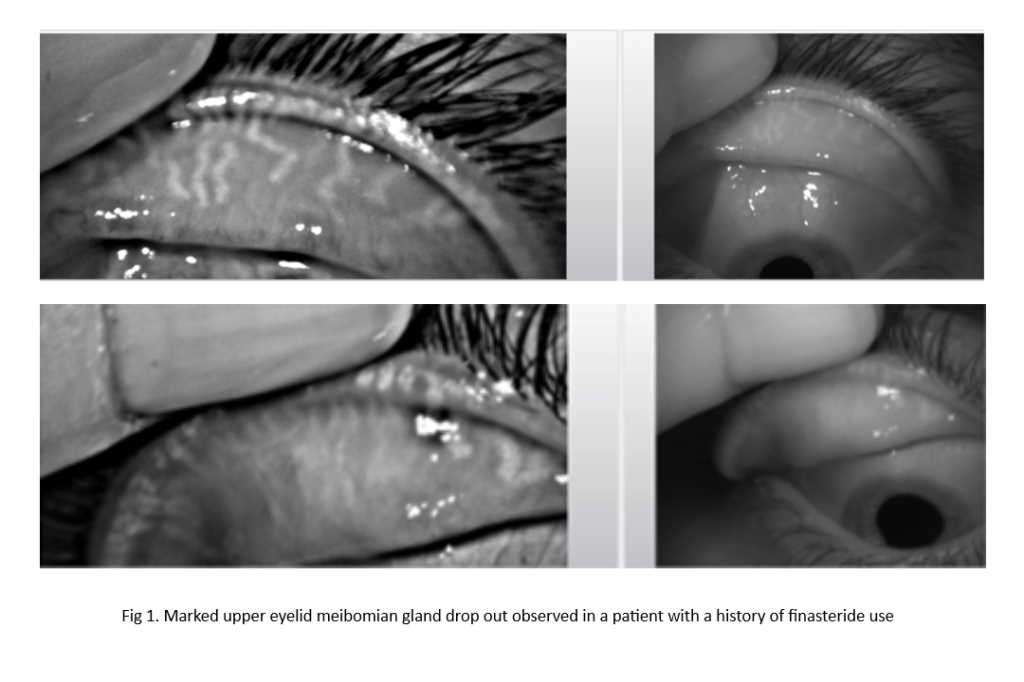
Slit lamp examination shows classic DED signs: nasal and temporal bulbar conjunctival hyperaemia; punctate fluorescein staining of the bulbar conjunctiva and cornea to varying degrees; lid margin telangiectasia, capped meibomian glands with poor, or little, expression of meibum; lid margin notching; and foaming of the tear meniscus along the lower lid. Keratography shows reduced tear breakup times and a poor-quality lipid layer. Tear osmolarity is also often elevated and meibography highlights significant meibomian gland drop out, with more than 50% of glands affected in the upper lid in at least one case seen in clinic (see Fig 1, above).
Ocular effects relating to finasteride use to date seem to be under-reported and poorly understood. Few studies have been performed, although one did show finasteride seems to affect tear production in rats4. Until more is known, however, it is worth considering the drug as a possible contributor to dry eye symptoms in patients, so clinicians are encouraged to carefully assess for symptoms and signs in patients who may be at risk.
In those affected, treatment may be indicated. Hot compresses have been shown to be effective in managing DED secondary to meibomian gland dysfunction, increasing meibomian gland expression across a wide range of severity8. Omega-3 supplements have also been shown to be beneficial in improving ocular surface health in a recent controlled study9.
References

Wendy Hill is a therapeutic optometrist based at Mortimer Hirst and Eye Institute in Auckland.