In the annals of history there exists a number of important discoveries that were conceived over a few beers. Arthur Holmes and his colleagues developed the theory of continental drift whilst sipping cocktails in Hawaii. Watson and Crick unravelled the mysteries of DNA’s double helix in the now-famous Eagle Tavern in Cambridge. Trivial Pursuit, the Iron-Man triathlon and even Harry Potter’s fictional sport Quidditch are all famous ideas that may not have come to be without the influence of a chilled alcoholic beverage.
The following innovation is not one of these.
Picture this scenario: On a balmy summer’s evening last year, a colleague and I decided a quenching ale was just the ticket after a long Friday of checking eyeballs. My final appointment of the day was a scleral contact lens fitting for a chap with advanced keratoconus. Once I had finished regaling my fellow optometrist with tales of the complexity of the case our conversation (rightly) turned to weekend plans. Given the heat, a swim at the local beach was on the agenda. “That patient of mine would have a tough time checking the water for sharks!” I laughed sympathetically. “Did you not design his sclerals to see underwater too?” my colleague retorted. Chuckles simultaneously turned to quiet speculation as metaphorical light-bulbs switched on above our heads. What if it could be done ...?
Water-wear
One of the few limitations of day-wear contact lenses are the difficulties when swimming. In my younger years I would dive and swim with lids clenched tight for fear of my soft dailies drifting away (Fig 1). Three years ago I had laser refractive eye surgery and still I get a guilty kick when opening my eyes underwater to experience the (blurry) wonders beneath the waves. This freedom is one of the main reasons I recommend orthokeratology lenses to patients who enjoy the water. Goggles are all good and well but they have their limitations: fogging of the lens, water influx, discomfort, field of view, and those lovely compression marks visible after removal. Plus, you’d never see a trendy surfer waiting for the next set with a pair of goggles strapped on. Wouldn’t it be neat if we could design a scleral lens swimming goggle that could offer great vision in and out of the water instead?
Several high-fives later we calmed down, ordered another round and extra napkins, and got serious. First things first: Would a scleral lens stay in an open eye underwater? We decided yes: the large surface area provides ample surface tension (when was the last time you were able to pull a scleral or hybrid lens straight off the eye with a suction tool? Clue: it’s not easy) and the lids should provide an additional barrier.
Second: How do we get around the issue of the vergence changes when a rigid contact lens is moved from air to water? As most of you will appreciate when underwater the human eye becomes severely hyperopic, by approximately 40 diopters, due to the cornea being almost entirely neutralised. A traditional rigid lens would behave similarly. Simply adjusting the contact lens front curvature to focus correctly underwater would lead to a colossal level of myopia when above the surface. Not ideal. One solution would to create a monovision-type set up, with one lens designed for vision in air and the other for vision underwater. Again highly impractical.
Eureka!
Then it hit us. Why not make a tiny goggle for each eye? Create the lens with a completely flat front and back surface, and insert the lens with an air gap, rather than filled with solution, so that the air/cornea refractive interface, and therefore the power of the eye, remained the same in air and water! In theory it would work perfectly. We left the bar that night with a sense of purpose rarely experienced by slightly-inebriated eye care professionals.
First thing on Monday morning I called Graeme Curtis at Contact Lens Corporation in Christchurch. “Was it even possible?” I asked. This lens would have quite possibly the flattest base curve ever created on a rigid lens, with essentially a radius of infinity. It is testament to the technology of modern day lathes (not to mention Graeme’s patience with seemingly foolish requests) that his reply was “Sure, let’s give it a try”. I heavily modified the parameters of a trial scleral lens using rigid lens design software Eyespace to match the cocktail napkin diagrams we had sketched previously. Regrettably ‘infinity’ was not a BOZR value I could input, so I had to settle on r = 99999mm. You read that correctly: Our lens had a 100 metre base-curve radius.
Weird science
As I opened the courier parcel from CLC you could have cut the tension with a knife. As it turned out the parcel’s contents; possibly the world’s first scleral swimming goggle, was the weirdest contact lens I had ever seen. The completely flat 6mm optic gave the lens a sinister appearance: It looked more like a part from a Terminator than something a water-sports enthusiast would wear. After the initial excitement subsided human trials began. Much like Australian Dr Barry Marshall, who drank a petri dish filled with the bacterium H. Pylori to prove the cause of stomach ulcers, in the name of science I bravely inserted the dry scleral lens onto my left eye.
Initial impressions were positive. For those of you who have not worn a well-fitting scleral lens they are surprisingly comfortable. I could feel this lens a little more than usual due to the abrupt junction at the optic zone edge but it was not irritating. And I could see! I could happily make out the 6/6 line on the chart due to my plano unaided refraction. Topography over the lens confirmed a front surface power equalling zero diopters; the lens was as flat as a pancake. OCT and anterior photography highlighted the unusual shape of the lens (Fig 3) and confirmed ~250μm of central clearance - important when the lens is 35D flatter than alignment.
However, things did not stay hunky-dory for long. After a few minutes my vision started to blur; I was struggling to see 6/12. Under the slit-lamp the rear surface of the lens was misting up like a bathroom mirror. We removed the lens and added a lubricant drop to the lens bowl prior to insertion. This helped for about five more minutes but the blur slowly returned. Only this time the lens was starting to become quite uncomfortable. Inspection showed the lens was fitting well in the peripheral area and still had adequate clearance. I managed to keep the lens in the eye for a further ten minutes, before the pain and significant blur necessitated removal.
We created a monster
Rather than relief, my first emotion was concern: the vision in my left eye was still very hazy: I was only reading 6/36 in my guinea-pig eye! The cornea was clear and uninflamed however instillation of sodium fluorescein revealed a subtle patchy negative staining of the central epithelium. Further investigation with corneal topography showed very irregular central mires (Fig 5). Realisation dawned: We had created a corneal exposure scenario mimicking the pathophysiology of patients with conditions like Bell’s Palsy, thyroid orbitopathy, restrictive eyelid disease and nocturnal lagophthalmos. Even a healthy eye with excellent tear film function will experience significant visual problems and discomfort when the lids are not regularly smoothing and spreading fresh tears over our fragile corneal surface.
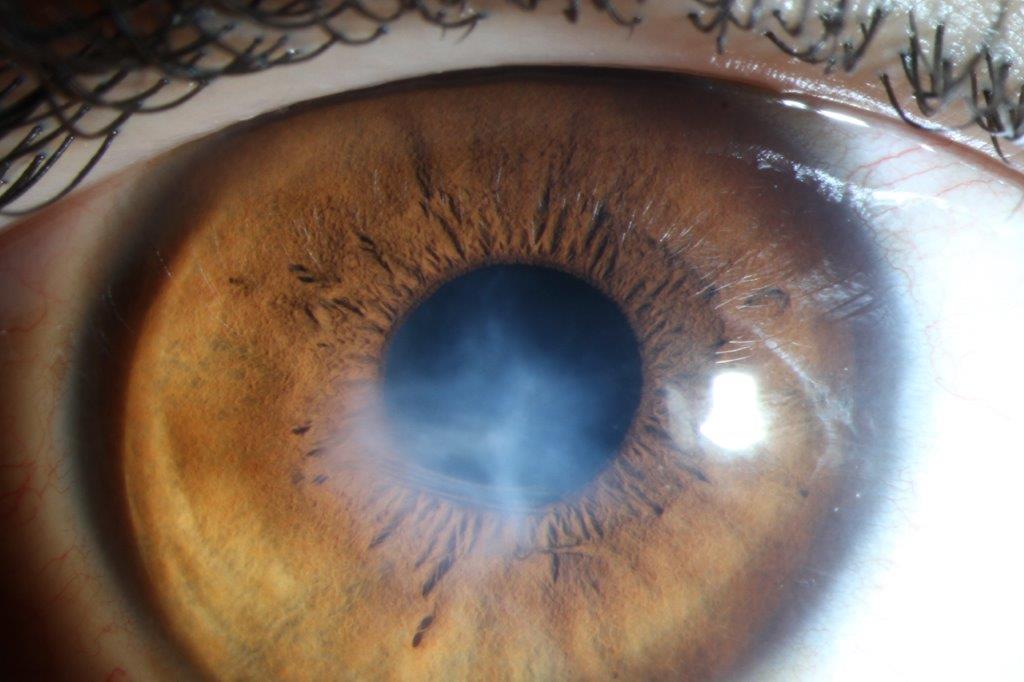
A case of one of my colleagues highlights this concept in a similar way: At routine aftercare a happy keratoconic patient noted that from time to time his lenses would be very painful and irritable for the duration of the day. The lens was fitting beautifully and in the chair his eyes looked pristine. The patient was asked to return wearing his lens if the irritation arose. A few weeks later the patient returned with a very red eye. One look explained his troubles: Poor insertion technique had trapped a bubble of air under his lens (Fig 6). As the bubble was for the most part off the optic axis he was unaware of it. Following removal, a kidney-shaped depression was evident at the site of the bubble, with dense epithelial staining within its confines (Fig 7). Needless to say it is important to educate scleral lens patients to check for bubbles after insertion with the aid of a mirror and sometimes a penlight. Like a stone trapped in a shoe, even a small pocket of air will gradually cause problems.
In the end it took roughly an hour for my vision to return to normal. Despite my scare I gamely tried the scleral lens one further time, except with a soft bandage lens worn beneath. The discomfort was not noticeable but vision became equally poor as the soft lens surface desiccated slowly. It was to be the last time that the scleral goggle would ever be worn.
Reinventing the wheel
The novel concept of using an air gap under the lens had ultimately proven the design’s downfall. So disappointing (and not to mention traumatic) was the outcome that the lens was never even tested underwater. With our luck it would have just floated off anyway!
It may seem like a waste of time to publish an account of this fruitless escapade. However, I think failures in science can also be viewed as learning opportunities. Rome wasn't built in a day after all. I discovered:
And perhaps the most important life lesson we glean from this tale: The grander a pub idea is; the more miserably it will fail!
On that sour note thank you for your support this year. Have a safe and happy holiday period. I look forward to entertaining with further specialty contact lens reports in 2017.

Fig 2: Is than an RGP lens? Or a pneumatic retinopexy gone wrong? No, this ladies and gentleman, is a scleral swimming goggle.


Fig 3 and 4: OCT and slit lamp appearance of the flat scleral lens profile on eye.

Fig 5: The exposure keratopathy induced by the air-filled scleral lens. Note the distorted mires seen on topography.


Fig 6 & 7: Epitheliopathy and inflammation caused by a trapped bubble under a well-fitting scleral lens. Images: Lachlan Scott-Hoy.
About the author
Alex Petty is a Kiwi optometrist who graduated from the University of Auckland in 2010. He has an interest in specialty contact lenses, ortho-K and silmoparis.com myopia control.