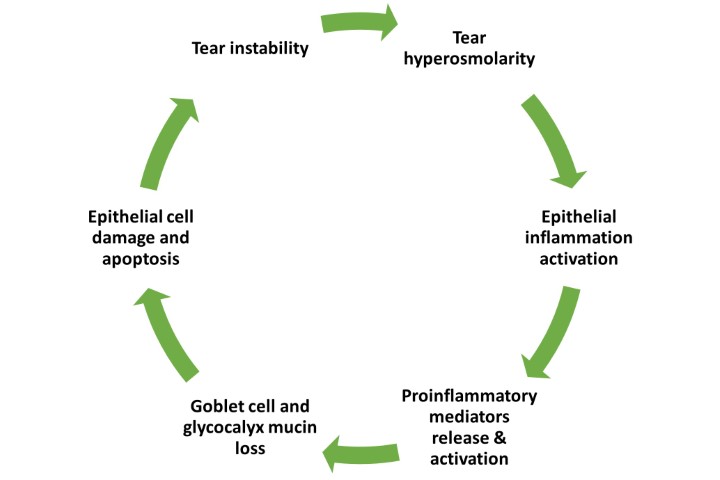
Inflammation plays a key role in triggering and propagating dry eye disease (DED) via the ‘vicious circle’1. In severe cases, topical anti-inflammatory therapy may be indicated, but managing a patient’s meibomian gland dysfunction can often be sufficient to resolve ocular surface inflammation without risking side effects from topical steroids2. However, accurately assessing ocular surface inflammation in clinical practice to inform management decisions can be challenging.
My master’s research project assessed the performance of a number of clinical methods for quantifying inflammation against levels of an established inflammatory biomarker, MMP-93, determined from conjunctival impression cytology samples by advanced laboratory analysis using droplet digital PCR (dd-PCR). The study included a total of 47 participants (37 with DED and 10 without DED, according to the TFOS DEWS II criteria). Those with DED underwent subclassification and all underwent inflammation assessment. The clinical tests of inflammation evaluated against the laboratory-determined MMP-9 levels included:
We found that subjective hyperaemia using the Efron pictorial grading scale, the objective hyperaemia assessment from Oculus K5M and the InflammaDry test showed the strongest prognostic values in detecting a ‘true’ raised MMP-9 level at the gene level. A cut-off score of >1 on the Efron grading scale was able to identify those with an upregulated level of MMP-9. Non-invasive tear breakup time (NIBUT), lipid layer thickness and both OSDI and DEQ-5 symptom questionnaire scores also proved useful in predicting elevated levels of MMP-9, allowing evidence-based cut-offs to be determined. Neither the ocular surface integrity measures using various vital stains nor the OSIE score were found to be predictive of raised MMP-9 levels.
This study highlights specific clinical parameters which might be relevant to consider when assessing and managing inflammation in practice, where it’s acknowledged that laboratory testing is not feasible. As MMP-9 is a non-specific inflammatory biomarker present in a wide range of ocular surface diseases, future studies might seek outcomes more specific to DED by investigating a wider range of biomarkers involved in the condition4,5.
References
1. Bron A, de Paiva C, Chauhan S, Bonini S, Gabison E, Jain S, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438-510.
2. McGhee C, Dean S, Danesh-Meyer H. Locally administered ocular corticosteroids. Drug Saf. 2002;25(1):33-55.
3. Lanza N, McClellan A, Batawi H, Felix E, Sarantopoulos K, Levitt R, et al. Dry eye profiles in patients with a positive elevated surface matrix metalloproteinase 9 point-of-care test versus negative patients. Ocul Surf. 2016;14(2):216-23.
4. Jackson D, Zeng W, Wong C, Mifsud E, Williamson N, Ang C, et al. Tear interferon-gamma as a biomarker for evaporative dry eye disease. Invest Ophthalmol Vis Sci. 2016;57(11):4824-30.
5. Tishler M, Yaron I, Geyer O, Shirazi I, Naftaliev E, Yaron M. Elevated tear interleukin-6 levels in patients with Sjögren syndrome. Ophthalmology. 1998;105(12):2327-9.

Catherine Jennings is a research optometrist and PhD candidate in the Ocular Surface Laboratory at the University of Auckland.