An 83-year-old retiree was referred to me for some assistance with reading. He told me on the phone about his long history of glaucoma treatment and discussions with his eye specialist indicated he had “reached the end of the road for treatment”. He was aware of reduced depth perception and concerned about the risk of falls. He was struggling to read and do crosswords but was quite enjoying listening to audiobooks.
As a result of his deteriorating vision, he and his wife were due to move into a retirement village and we agreed to hold off meeting until they were settled there.
Meanwhile, the ophthalmologist’s referral confirmed the history of primary open-angle glaucoma (POAG) with bilateral trabeculectomy, ongoing medication for the right eye, bilateral pseudophakia and, surprise, dry macular degeneration (AMD). The patient is virtually emmetropic in the right eye and has a moderately myopic left eye (-2.00/-1.00 x 90) using a single-vision distance prescription and reading unaided. My suspicion was that this prescription was originally a monovision outcome of cataract surgery performed a number of years ago, before a right non-ischaemic central retinal vein occlusion reduced his distance vision to hand movements and forced him back into spectacles for distance.
When I mentioned that his reading was now being affected more by AMD than glaucoma, he and his wife, who attends his appointments with him, appeared to be in shock at the revelation of the additional diagnosis of AMD. Had they really not been told of this or had they failed to take it in when it was explained?
It is my long-held belief that helping a patient understand the functional changes they may experience as a result of their optical and general medical history reassures them and their whānau that they are not imagining problems. Nor are they alone in their battle to live with these issues.
Glaucoma, in particular, is always considered a medical problem. Consultations revolve around the results of tests to ascertain deterioration and treatment options to manage it. There is seldom discussion on the functional effects of glaucoma on daily living, or suggestions as to how to minimise the discomfort or disability that the medical issues create.
Throw into the mix a further diagnosis of AMD and a wife who is anxiously trying to cope with taking over and making adaptations for a future with a ‘blind’ husband and there is more than a reading problem to sort out. First, I had to explain central and light vision operated mainly by the macula, then peripheral vision and darkness vision more affected by glaucoma.
The patient’s wife’s jaw nearly dropped to the floor as she emotionally told me they had recently gone out for a special dinner to a restaurant in an unfamiliar area. She had only found parking in a dark side street. When the 83-year-old patient tried to get out of the car, he found he was unable to see anything at all. With a rising sense of panic that “this was it” they both stumbled along the path until his vision gradually started to return. Their pleasant evening turned into a nightmare.
My explanation of light/dark adaptation, with common examples of other people’s experiences and ideas for avoiding similar situations in the future, offered them huge relief.
Next was a discussion on loss of contrast and how even the best-managed cases of glaucoma can still affect contrast, particularly when combined with macular problems and/or cataracts, corneal haze or neurological problems (often not taken into consideration).
When it comes to reading, the loss of contrast can frequently have a greater effect than the size of the print. My client confirmed the former was exacerbating his reading problems and impacting his depth perception. His consequent loss of confidence walking unaided, one of the few pleasures left to him, prompted the couple’s decision to move into the retirement village.
Patients with glaucoma are frequently troubled by glare problems. This can mean reduced acuity or discomfort on the spectrum from hardly noticeable to quite disabling. Becoming aware that there is a connection between their sensitivity to indoor or outdoor glare and their diagnosis of glaucoma is often a complete revelation to patients.
The double whammy of glaucoma and AMD
A person with macular problems needs extra light, but the glaucoma person is wearing dark glasses, turning off the lights and pulling down the blinds. The solution to this dilemma is to first explain the problem. With greater understanding comes greater acceptance, reduced anxiety and greater openness to finding solutions that work for that individual.
My assessment of my client revealed that he was not blind or ‘end stage’ – two emotionally charged labels that add nothing to a patient’s understanding of how to live with their ocular history, other than copious quantities of anxiety.
Binocular functional visual fields showed he had a partial ring of absolute scotoma between 5° and 10° from the fixation point in his inferior field, extending around to his left field narrowing over the horizontal and extending to about a 45° angle in the left superior field (Fig 1).
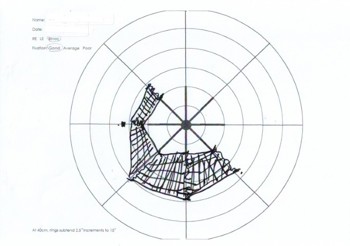
Fig 1. Binocular functional visual fields showing a partial ring of absolute scotoma
between 5° and 10° from the fixation point in the inferior field
This would result in considerable problems in mobility and may present a significant risk of falls. Once again, showing him the evidence of this confirmed his experience and enabled a discussion of awareness and avoidance actions.
Binocular near acuity was N8 on a high-contrast single-word reading chart in average room lighting. This improved to N5 with intense local light and improved further to N4 (!) with a continuous text reading card. His low-contrast acuity, however, was reduced to less than N80.
With this information, it was easy to see that this man needed minimal magnification as long as he had high-contrast materials enhanced by the right light in the right place at the right time. With this understanding, my retired electrical engineer was able to quickly rearrange the reading lamps in his new apartment, discarding those that were unsuitable. He also purchased a pocket-sized LED-illuminated magnifier to give him greater independence in shops, restaurants and signing documents, etc. and a couple of small LED torches to keep in his pocket to assist him in poor light, since he doesn’t carry a mobile phone.
As his wife insisted on accompanying me to my car, she confided she was becoming desperate as her husband became increasingly withdrawn and perhaps depressed at his increasing dependence on her. She felt that our (admittedly long) session together had already made a difference to his demeanour and might allow her to step back somewhat and enjoy the activities available to her at the village. The lack of information and understanding of his visual problems had eroded the patient’s self-confidence to the point that it was starting to impact their quality of life.
Perhaps the take-home message is that patients and their families need more than a diagnosis to help them to adapt to living with low vision. They need to be encouraged to bring a support person to consultations to take notes, ask questions and help them to remember what was said. Beyond being told about the treatments available to them, they need information about how each condition may affect how they’ll see in the future and the strategies and devices available to them continue to use their remaining vision more efficiently and comfortably.
However, such information cannot always be delivered within the time constraints of a single consultation. That is where peer support groups such as Macular Degeneration New Zealand, Glaucoma NZ and Retina NZ can play a huge role. Often patients are incredibly relieved just to talk to someone who understands what they are going through and can explain in layperson’s terms what the diagnosis means. Misinformation from well-meaning friends and relatives can be devastatingly destructive.
Recognising that chair time is a limited and expensive resource, we have to be able to acknowledge the importance of assisting the newly diagnosed patient, or those with a significant change, to access additional support and rehabilitation services to make the best of the vision they have, rather than focusing on what they have lost.

Naomi Meltzer is an optometrist who has recently retired from running an independent practice specialising in low-vision consultancy. She is a regular contributor to NZ Optics.