


Coinciding with leaves changing colour in the beautiful grounds of Remuera Golf Club, Eye Doctors’ first Grand Round is a trusted autumn calling card. While guests enjoyed a delicious dinner, practice manager Shellene Garofalakis welcomed everyone with a quick-fire quiz to switch our brains into gear.
Next, Dr Arvind Gupta delved into idiopathic intracranial hypertension (IIH). While this chronic condition is rare in the general population globally, it is much more common in this part of the world due to a genetic predisposition. Most patients (>90%) are female and within reproductive age, with the most commonly presented symptom being headache, typically in the early morning. The most common ocular sign of IIH is bilateral disc oedema.
The condition is associated with a high body mass index (BMI) and, for many patients, its impact tends to fluctuate over time with lifestyle changes and medication. Dr Gupta said there is also a very small group of atypical patients he sees where headaches and optic disc oedema are absent, but with transient visual obscurations (70%), back and neck pain (50%), pulsatile tinnitus (>50%) and some (10–20%) who are completely asymptomatic.
Pseudotumor cerebri (PTC) has the clinical features of IIH but is due to a secondary cause, with or without obesity. Medications known to elevate the risk of developing IIH include tetracycline antibiotics (eg. minocycline, doxycycline), ciclosporin (immunosuppressant), sertraline (anti-depressant) and topical retinoic acid (for acne treatment). These patients typically present with a sudden onset of symptoms with rapid improvement after removal of the offending factor.
There was a discussion about the new weight-loss drugs (glucagon-like peptide-1 receptor agonists) available and their role in lowering BMI. Dr Gupta agreed that while patients are on the drugs, they appear effective and also help bring the disc swelling right down but there are other side effects and a lack of long-term data, he said. More on this in May’s issue of NZ Optics.

Dr Arvind Gupta with Jason Ku and Neha Kumar
ROP – our tiniest cohort
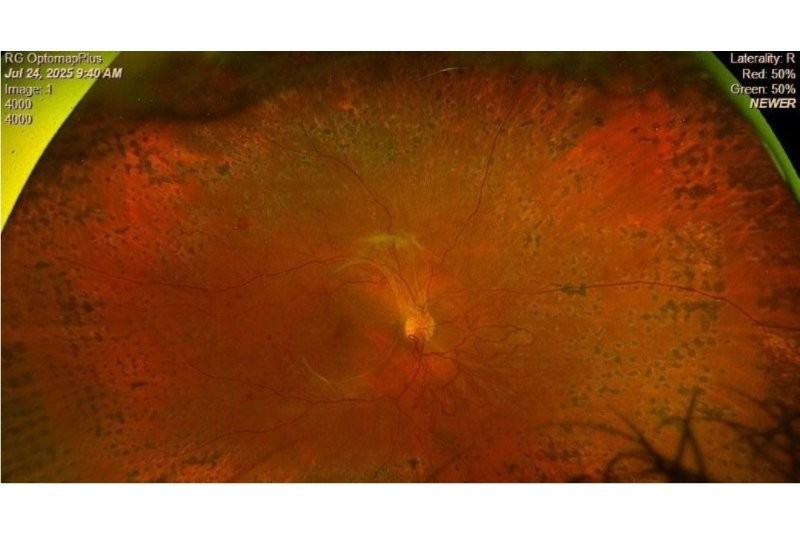
Dr Julia Escardό-Paton presented an update on retinopathy of prematurity (ROP), a proliferative retinal vascular disease where the blood vessels grow into the vitreous rather than into the retina. Walking the audience through the intricate and precise development of the eye in gestation (starts at week three), classification of ROP and screening, Dr Escardό-Paton then focused on treatment.
Fortunately, fewer premature babies are blinded from ROP nowadays (an 80% reduction 2012–2024). Historically treated with cryotherapy, ROP is now managed with laser or intravitreal anti-VEGF (0.05ml – half the adult dose). As with most things medical, there are advantages and disadvantages with both, said Dr Escardό-Paton. While being more definitive and carrying less risk of recurrence, laser is a difficult and long procedure (both medically and logistically); it also permanently destroys the peripheral retina, so there is no chance of further vascularisation. Moreover, it’s not effective for all types of ROP, such as aggressive cases, and is associated with a high incidence of myopia later in life, she said. Anti-VEGF, on the other hand, is a quick procedure that delivers a rapid effect and allows for continued vascularisation of the retina. While it delivers less myopia risk, it adds risk of endophthalmitis, cataract formation, retinal detachment, reoccurrence of disease, unusual vascular abnormalities and requires much longer follow-up compared with laser. There may also be unknown developmental effects, she added.
Long-term conditions resulting from ROP include refractive errors (myopia), strabismus (14.3% of those treated for ROP at one year old), glaucoma (due to shallow anterior chambers (AC) in presence of stage 4 or 5 ROP, shallow AC and myopia) and retinal detachment.

Georgia Cheng and Kevin Lee
Just a floater?
There is a clinical shift happening now where vision-degrading myodesopsia (floaters) is no longer regarded simply as a nuisance but a recognised functional impairment comparable to AMD and diabetic retinopathy, said Dr Mark Donaldson.
The impact on quality of life is particularly true for multifocal IOL patients, who struggle significantly more with neuroadaptation compared with those with monofocal lenses, since the former reduce contrast sensitivity by about 25%. “When multifocal-related glare and halos meet posterior vitreous detachment-induced scattering, the cumulative contrast loss can be debilitating,” he said.
Having ruled out other pathology (tears/detachment) with a 360° depression, Dr Donaldson manages these patients in a stepwise approach, giving them the Royal Australian and New Zealand College of Ophthalmologists’ advice on flashes and floaters and educating the patient on neuroadaptation (the brain can filter out stable shadows in three to six months). There is also some evidence to suggest micronutrient formulations (L-lysine, vitamin C and grapeseed extract – VitroCap N) may reduce the opacity area and improve visual comfort (Flies trial), he said. Ultimately, for refractory issues with a high impact on quality of life, pars plana vitrectomy is the definite solution but it comes with its own risks, in the form of retinal detachment (~30%), cataracts (~20%), elevated IOP (~20%) and more.

Lahiru Gunasena and Richard Johnson
Lastly – intrigued by new aids on the market such as Nuance and bone-conduction hearing aids – Dr Andrew Riley concluded the evening with an entertaining talk on hearing loss. Bringing clarity to the double sensory shift optometrists deal with on a daily basis – presbyopia and presbycusis (age-related hearing loss) – he added there are some real red flags to watch out for, including sudden hearing loss, discharge, vertigo and pain.
The next Eye Doctors’ Grand Round is pencilled in for 26 August 2026.